Using Patient-Specific Data as a Basis for Design, 1 in a Series
Integrating anatomical STL files with RP and manufacturing to create a 3D reconstruction.

Latest News
June 26, 2008
By Susan Smith
 Alair Emory, Sr. Partner, Javelin 3D, (Park City, Utah) heads up digital design and development for Javelin 3D, which specializes in anatomical 3D reconstructions and medical models.
Alair Emory, Sr. Partner, Javelin 3D, (Park City, Utah) heads up digital design and development for Javelin 3D, which specializes in anatomical 3D reconstructions and medical models.
Emory, who holds both chemical engineering and biology degrees, bought her first rapid prototyping machine in 1991 and founded Javelin 3D, Image3 LLC and BodyReplicas thereafter. Also a co-developer of Velocity 2 Software, a package that imports grayscale, Emory makes the disclaimer early on that she does not sell or represent CAD programs, viewers or file conversion software.
Her paper at RAPID 2008 focused on the topic “Integrating Anatomical STL Files with CAD” in which her goal was to be able to use patient specific data as a basis for design. “I have clients who would like to be able to use this data in their CAD program – they’re only asking for use of part of the spine, to be able to cut and drill holes in the spine and fit their devices to these geometries. This is still very difficult, expensive to do and in some cases, not possible.”
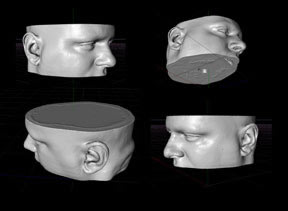
Emory said her company uses software that will import medical scan data. For vertebra, this would be CAT scan data as it is the best for bone. “Each scan slice is essentially a black and white picture of a slice of the anatomy. The software allows the user to identify the anatomical region of interest and then links each slice together in 3D to reconstruct the identified region,” she said.
 By using Javelin 3D’s Velocity2 software, users can achieve an STL with Dicom, Tiff, or other proprietary 2D grayscale image data, and do segmentation, 3D reconstructing, smoothing and file size reduction all within the same program. Emory said there are other programs that can do this: 3D Doctor is a good program created in the U.S. by Dr. Ted Wu. Another software with the “most advanced options” is Materialise with their Mimics software, plus they have some surgically integrated software.
By using Javelin 3D’s Velocity2 software, users can achieve an STL with Dicom, Tiff, or other proprietary 2D grayscale image data, and do segmentation, 3D reconstructing, smoothing and file size reduction all within the same program. Emory said there are other programs that can do this: 3D Doctor is a good program created in the U.S. by Dr. Ted Wu. Another software with the “most advanced options” is Materialise with their Mimics software, plus they have some surgically integrated software.
Emory gave a definition of STL files for creating 3D reconstructions of anatomical parts for that purpose as follows:
- Tessellation language refers to the representation of 3D forms constructed entirely of triangular facets.
- STL files describe the surface geometry of a 3D object without any representation of color, texture or other common CAD model attributes. The STL format specifies both ASCII and binary representations.
- State of the art 3D reconstruction software packages can be used to create STL files.
- CAT scan data is not considered 3D data for CAD packages.
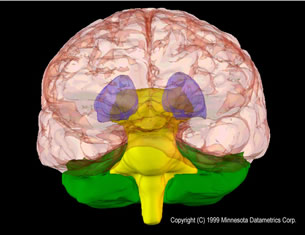
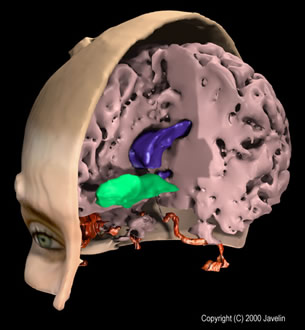 Composite of structures in the human brain as reconstructed from MRI data. 3D Files were exported from Velocity2 PLUS and image was rendered via 3D party software. (Reconstruction courtesy of Javelin, Salt Lake City, UT) |
Once you import your 2D gray scale data and work with the reconstruction of the brain, or whatever anatomical part you are working with, you seek the tissue you’re interested in reconstructing within your data.
Emory said that medical reconstruction is not well integrated with rapid prototyping.
“Often you’re working with a radiologist or surgeon who only knows about a Dicom format, nothing else,” she said. “3D image reconstruction programs exist for visualization purposes, but are not well integrated with RP and manufacturing.”
A multidisciplinary background is needed to be able to make the link between RP and medical product development. Besides this issue, there are other challenges:
- The Dicom format was standardized within the medical community
- Free medical viewers
- Health insurance and litigation issues
- Medical community’s AMA standards and requirements.
How do you get around these challenges and/or make use of the knowledge base that already exists? Based on experience, Emory has developed a number of tips and tricks and approaches.
Emory suggested the “Medical 3D Approach:”
- Obtain smallest possible file size without losing important details.
- Find ways to communicate geometry details across multi-disciplines. STL file viewers are wonderful for that.
- Define CAD Conversion software requirements necessary to drive medical applications forward.
Emory evaluated the following types of programs:
- STL File Viewers
- STL File Size reducers
- Standard CAD and
- File conversion programs
“I used a sample STL file I had reconstructed from CAT scan data, 18.2 MB,” said Emory. In evaluating the products, she approached the companies directly and/or downloaded software in demo, shareware or freeware format.
STL File Viewers
What Emory looked for in evaluating STL file viewers were the following features:
- Easy to install
- Able to handle large files
- Include measurement features
- Low cost or freeware
- Able to print 2D views
- Runs on “basic” PC
It is important to have the ability to print 2D views because the medical community can easily view them. These do not have the ability to reconstruct and save to a 3D format. If you tell them you are sending them a 3D file they have to look at in a viewer.
Emory has some favorite STL file viewers – MiniMagics by Materialise is top of the list. Other choices include shareware such as Quick3D which has “confusing zoom control but good customer service.” I-know 2Deasily generates 2D technical drawings and measurements but is not freeware.
Anatomical STL File Size Reduction
For medical rapid prototyping, file size reduction should be done directly in the package that you’re generating the file in, according to Emory. “If you’re working in medical RP you shouldn’t use secondary file size reduction programs.”
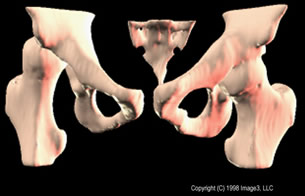 Reconstruction of CT image data of a young patient with congenital hip dysplasia (approx. 50 slices). (Data courtesy of Shriners Hospital for Children, Minneapolis, MN and Image3, LLC, Salt Lake City, UT) |
There are some legal reasons for this. “When you go to third party software packages that do STL file reduction, you don’t get input back in general as you do in the medical RP package,” explained Emory. Also, “You shouldn’t get rid of the medical data form file (the industrial engineer may want to do that – how would they decide what is the most important aspect of anatomy to keep or not?)”
Because anatomical files are detailed, if you get a medical STL file, you need to tell the person doing the reduction what your needs are. Emory also counseled, be careful as you reduce the file size you are reducing the number of triangles.
As a member of SME’s RP medical committee, Emory said the issue of file reduction of medical files is under discussion. “If you are working with an industrial part - say it is a design for a cell phone case cover and a RP service bureau gets the STL file with a request to build the prototype it would be common for the service bureau to run the industrial file through a file size reduction operation before building the prototype. Often industrial designers will save their designs as very large files. The service bureau wants to reduce the file size because large files can be difficult to pre-process for the RP build operation. With an industrial part it would be pretty easy for the RP operator to visually look at the original file and a size reduced file and give the go ahead to process the build.”
“In general, medical STL files are large and the concern is that the RP service bureau operator is automatically going to want to reduce the file size. However, what might not seem important to the RP operator might actually be important to the medical diagnostician. If the medical STL files go through file size reduction, important anatomical data might be lost. It seems that the best option would be to create a standard for medical STL files that restricts file modifications to the originator of the file. The service bureau should not modify the file in any way unless they created it in the first place.”
An example of a standalone reduction is VizUp which can also serve as a viewer.
CAD Programs
CAD programs used commonly for anatomical STL include SolidWorks and Pro/Engineer. Rhino from Robert McNeel & Associates is also very capable.
The recommendation from SolidWorks technical support is that anatomical STL files be processed by third party software conversion programs before import into SolidWorks.
Rhino was “most responsive,” according to Emory. “Technical support claims import into their program without problems, and we were able to demonstrate import of vertebra file into the Rhino Software.” In spite of this, Emory said they did not have any clients using Rhino.
 A plastic soap dish, varying in thickness from 1.5 to 3.5 mm, was scanned in a hospital CT scanner (approx. 200 slices). Using Velocity2 Pro, a reconstruction was made in less than 10 minutes and a prototype built on an FDM machine. (Data courtesy of Lonepeak Engineering, Salt Lake City. UT) |
Pro/Engineer has a reverse engineering module and contains licensed code for surface fitting which is a kernel within their base code. “We were able to put together a demonstration for numerous modifications to a jaw stl file provided for a dental webinar,” said Emory.
Although Pro/Engineer represents the right approach for medical RP, it is a difficult package to work with. Emory reported that the dental surgeon working with it was discouraged by cost and the complication of the software.
Conversion Programs
According to Emory, conversion programs are costly but do provide valuable solutions.
SolidWorks recommended the following: Geomagics – to work with anatomical stl file conversion to NURBs you should only need 2 modules. You do need a specific graphics card. NuGraf (Okino) with many output options, and Rapidform.
In conclusion, Emory stated that the area of medical RP is still very confusing to a lot of people. Some programs simply don’t work and solutions are still expensive. She suggested that the SME RP Medical Group should develop standards to be met for the utilization of medical RP data. Her suggestions include:
- guidelines on medical RP file modifications
- guidelines on conversion of these files to other file formats for use with standard CAD programs or FEA analysis
- guidelines on quality of original medical scan data
- recommendations on appropriate use of RP systems. Some RP systems are much more accurate than others but medical practitioners can get confused by all the options.
- recommendations on use of 3D physical medical models in the operating theatre. RP models have been used regularly outside the US in the operating room. A summary of this with information on sterilization methods/options and helpfulness to the surgeon would be valuable to have as a reference.
For details, contact Javelin 3D.
Susan Smith is a contributing editor for Desktop Engineering magazine. Sende-mail about this article to [email protected].
Subscribe to our FREE magazine, FREE email newsletters or both!
Latest News
About the Author
DE’s editors contribute news and new product announcements to Digital Engineering.
Press releases may be sent to them via [email protected].